Home › Forums › General Discussion › Bloodwork – herxing/SD related, or something else (Multiple Myeloma)?!
Tagged: scleroderma, Lyme, multiple myeloma
- This topic has 20 replies, 4 voices, and was last updated 3 years, 9 months ago by
stevewrightfilmmusic.
-
AuthorPosts
-
June 3, 2020 at 2:50 pm #465795
stevewrightfilmmusic
ParticipantHi everyone,
A while ago I posted on here regarding my mother in law’s dizziness, and whether it could be related to her Thyroid and LDN. It turns out it could be Thyroid related after some bloodwork was done, however a number of other things came up on the bloodwork, which I would love your opinions on. Our problem is that the doctors here in Ecuador really have little knowledge or understanding of AP treatment for conditions such as Scleroderma, and they dont really acknowledge Lyme disease as a precursor to AI disorders/chronic infection that can wreak havoc all over the body. Therefore, discussing the bloodwork with the docs here can be a little one-dimensional – with no disrespect to them, but they simply don’t consider certain potential causes/factors because they don’t practice the therapies here, and in some cases dont even acknowledge the conditions…
She has a Lyme specialist in CT who is great, but we similarly feel that given his specialism is in Lyme, not SD specifically, and similarly not in the conditions that the Ecuadorean doctors are hinting might be happening, we want as many opinions as possible to combine with what the various docs say. Sorry for the complicated nature of my introduction, its very hard for us to determine how to approach things..
To get straight into it, her Total Serum Protein was slightly high on her most recent results (9.05, ref range being 6.6-8.7g/dL), as well as her Monocyte levels being a bit low (3.1%, ref 5-11%), and she was showing as being anaemic (we know about the anaemia already). We received a call from a doctor at the lab who brought to our attention that these sets of results *could* be indicative of a condition ‘similar to leukemia’ (he was very vague frustratingly), and suggested we have a consult with him, and run two additional tests: Protein Electrophoresis and Beta 2 Microglobulin tests.
Having done a bunch of reading online, the only condition that really matched her results, and what he had said with reference to Leukemia, and the tests he suggested, was Multiple Myeloma. Of course immediate panic, Scleroderma and Lyme is enough for anyone in one lifetime! Her other results didn’t line up with Leukemia, or any variant, given what we had read (her Neutrophils, Lymphocytes, Eosynophils, Basophils all normal), and the two additional tests (Electrophoresis of Protiens and B2B tests) led us to the conclusion that he was probably referring to MM.
That being said, her symptoms don’t really line up, and other blood factors didn’t line up with this possible diagnosis. More specifically…
– Bone Pain, especially in chest and back – she does not have this ever, and in general no bone pain. Pretty much the only pain she experiences is the neuropathy in her feet and right hand
– Nausea – never experiences this (apart from when she eats too much sugar free chocolate!!)
– Constipation – again not an issue, she is going more than she ever has!
– Loss of appetite – her appetite is also better than it ever has been, and she is on a very healthy diet too these days.
– Mental fogginess or confusion.. not specifically, she is tired and dizzy, but not confused.
– Fatigue – yes she has this, but presumably due to the anaemia?
– Frequent infections. She often gets puss on the tips of her fingers, in the sores of her skin. She has had this for many many years, part of the Scleroderma. Body-wide infections (bladder, chest, throat, etc) – practically never.
– Weakness or numbness in legs – yes this is something she has, but due to the neuropathy (and she suffered a stroke last October so her stability is still lacking, getting better though…)
– Excessive thirst – she is occasionally very thirsty, typically after food. She has never drank much water, which we are now putting right. As a result, thirst much better.In terms of blood, in addition to the above mentioned diagnostics of Total Protein and Monocytes, you may also find the following, according to various reputable online sources:
– Creatine; could expect to be high if suffering from MM due to kidney function. She has normal Creatine (0.86, ref 0.5-1.4 mg/dL)
– Albumin; could be low with MM… hers is normal (3.96, ref 3.5-4.8 g/dL)
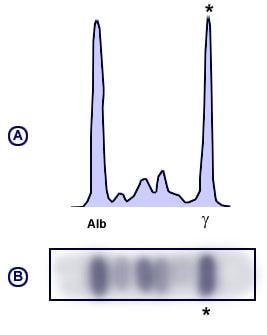
– Calcium; high levels in advanced MM – she has normal Calcium (8.7, ref. 8.4-10.2mg/dL).We got the Protein Electrophoresis and Beta 2 Microglobulin results back, and they are somewhat inconclusive. As would be expected in MM, there is a raise in the gamma region, but it isn’t a huge ‘church spire’ spike as many of the online references suggest. In fact, Medscape has the following explanation:
Monoclonal gammopathy
A dense narrow band that is composed of a single class of immunoglobulins secreted by an abnormally expanded clone of plasma cells is known as M-protein (paraprotein, monoclonal protein, or M-component). [3, 4] An M-protein usually presents as a single narrow peak, resembling a “church spire,” in the gamma, beta, or alpha-2 region of the densitometer tracing, or as a dense, discrete band on the agarose gel (the graph trace looks like this: https://img.medscapestatic.com/pi/meds/ckb/31/14031.jpg)Polyclonal gammopathy
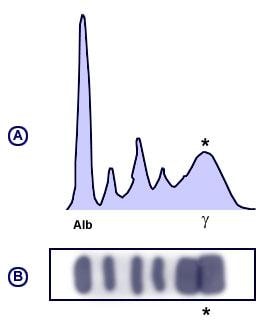
Infectious, Inflammatory or various reactive processes may be associated with a broad-based peak or band in the gamma region (Figure 4). This pattern suggests a polyclonal increase in immunoglobulins. Liver disease, autoimmune disease, chronic viral or bacterial infections and various malignancies may cause a polyclonal rise in the gamma fraction (the graph trace looks like this: https://img.medscapestatic.com/pi/meds/ckb/30/14030.jpg).For your reference, I have attached an image of her trace if you go to the following link (dropbox link: https://www.dropbox.com/s/2tlcf8vd86122z7/Screenshot%202020-06-03%20at%2011.08.11.png?dl=0)
For me, her results resemble the description/image of the ‘Polyclonal gammopathy’. Reading further, A Polyclonal gammopathy can be caused by the following conditions:
Cirrhosis, autoimmune or viral hepatitis, Rheumatoid arthritis, systemic lupus erythematosus, scleroderma, Sjogren syndrome…
The list goes on, but most significantly, Scleroderma and Sjogrens are listed.
OK, so that concludes my crude and lay-man analysis of the situation. I then did a search of this forum, and found the following quote from Dr Brown:
https://www.roadback.org/index.cfm?fuseaction=studies.display&display_id=184#Anchor-The-51540
Laboratory tests can help differentiate between a worsening of disease (RA flare), a Herxheimer reaction to microbial toxins, and an allergic reaction to medication.
1.WBC will elevate in a Herxheimer and lower in a flare.
2.A Herxheimer will also exhibit a coincidental elevation of SED rate, gamma globulin and total globulin, and a fall in serum albumin and hematocrit. Patients who exhibit this flare reaction accompanied by anemia, depression of serum albumin, elevated total globulin and gamma globulin are probably reflecting a more intense reaction pattern to anti-L substances than in hematologically mild cases.
3.A marked increase in eosinophils (for instance about 30%) is an indication of an allergic reaction to the drug.Comparing to her results, this is perhaps the most interesting find of all…
1) Her SED rate is up, 33 (normal being up to 29 for women)
2) Her Gamma Globulin is up
3) Her albumin is normal on on one set of results, a little low on another? (they use different reference ranges).
4) Her Hematocrit levels are low (28.5%, ref. 38-47%)
5) She is anaemic, and her bloodwork suggests this too at this time.Another oddity was that in the initial test results, the reference range for Monocytes is 5-11% (her level is 3.1%). However again looking at many resources online, they state the reference value is more like 2-10%. So according to this lab, she is low, but according to other sources, she is ‘OK’.
She started AP back in January with 2x 100mg Minocin every day, and a month later introduced Bactrim, twice a day. She was also on a variety of Antimicrobials prescribed by the Dr. She has suspended them temporarily whilst we try and figure out her dizziness. She was definitely herxing – a rise in the Antimicrobial dose coincided with increased intensity of pain, body wide. This would subside a few days after a few days at new dose, but kick in again when we increased the dose 5 days later. It seems more than a coincidence that Dr Brown’s quote coincides with her bloodwork.
And BREATHE!!
OK if you’ve got this far, first of all thank you. You might be thinking why I don’t just go to our doctors to discuss this. Well as I explained before, the doctors over here are not familiar with AP, less so with a Herx reaction, and therefore even less so with the potential effects a Herx can have on bloodwork. Hopefully they will be familiar with the nature of the gamma ‘spike’, and the differences that I showed above and what that can indicate. Similarly, our Lyme specialist is really great, but I’m not sure how much of this detailed bloodwork is relevant to his field of specialty (obviously it is if it is caused by the Herxing/a typical sign of an AI condition, but it may be a little less his area if we are talking more about Multiple Myeloma).
Another thing to add – the Dr who works for the lab, who initially suggested we run the extra tests, probably knew very little about my mother in law’s medical situation/history. We did not go through her usual State-ran doctors/hospitals with which she is affiliated, as we are not risking going near the hospitals right now with her, and they don’t offer a home service. We therefore paid to get these done privately, but as a result there are no records in their system of my MIL. He therefore made this suggestion/judgement based purely on this one set of labs (ie he had no context of what she is currently suffering from). We have notified him of this, but again without wishing to come across as sceptical or rude, we are constantly questioning the broader knowledge the Drs have over here, especially in complex cases such as my MIL.
We are talking to this Dr later today, he may well be fully aware of this and have a very sure answer for us, either way. But given the number of extremely knowledgable and experienced people on this forum, who have access to the very best Drs in the world, we would love anybody’s second opinion/personal experience. Granted many of you may not be qualified Drs, but I think its dialogue such as these which actually lead to the truth (perfect example being that MIL was undiagnosed of Lyme for 30 years given the lack of attention the Drs over here give it, and due to this forum we finally got that diagnosis confirmed!) We are of course also following up with our Lyme Dr in CT to see what his opinion might be.
Thank you everyone, and I’d like to say a special thank you to Maz who, I think we can all agree, is a beacon of support and hope and care and love to all of us, ourselves included.
---
Here for my Mother In Law.
Scleroderma 30+ years, Lyme/Bartonella (perhaps 30+ years too, diagnosed in October 2019), Hypothyroid, Anemia (of chronic diseases we think?), Neuropathy, Mini-stroke/brain lesions Oct 2019, Candida.
Current Meds:
**Minocin 100mg x2 day, every day. **Rifampin 300mg 1x day MWF. **75mcg Levothyroxine. **5mg Prednisone. **Clopidogrel 75mg. **300mg Fluconazole every Sunday. **300mg Gabapentin. **LDN 4.5mg.Current Supps:
Vitamin B-complex, C, D, E. Potassium GluconaJune 3, 2020 at 7:40 pm #465798Linda L
ParticipantDizziness is one of the main symptoms of B 12 deficiency. Note that the levels recommended by our authorities levels are far too low.
RA tried everything: Methotraxate, Arava, Humira. Pneumonia three times. Anemia. Very low iron. Hypothyroidism
AP from April 2014 till August 2015. No luck.
Current medications: Natural thyroid, Mobic, supplements,
vitamins and minerals.
MTHFR heterozygousJune 3, 2020 at 10:39 pm #465799Vincentpre23
ParticipantHi Steve ,
I don’t have much to add other than I looked back at my tests and did notice my rheumatologist ordering the Protein Electrophoresis lab when she suspected I had scleroderma. I think in general there is a higher risk of cancer in sCleroderma . My values were normal so I didn’t really ask her to explain the results or reasoning behind the test . Hope you get answers soon .
4/19 symptoms onset
UCTD , 1:40 ANA Speckled, Now negative
Mycoplasma P IGG IGM, EBV, HSV1, Igenix Bartonella IGG
Doxycycline 100mg b.i.d. , Bactrim ds 960 mg b.i.d. , Biodisrupt, fluconazole 100mg q.d , Monolauren, Visbiome probiotic 112.5b b.i.d ,B-complex, Vitamin D , Quercetin, saccharomyces boulardii, raw garlic , paleo, WHMJune 4, 2020 at 8:18 am #465801ParticipantHi both,
Thanks for your swift replies. Linda yes I saw your post in the other thread. I checked her results, her B12 seems OK (it’d well within the range, but as you say the recommended range is very large. It’s towards the top end, so I shouldn’t think thats the issue?)
As for the Electrophoresis, we were able to speak with the Dr who made these recommendations (note that we have no idea who he is – I think he just works for the labs to do a complimentary check over the results, and then notifies the patient if anything seems untoward). He, like me, didn’t feel that the shape of the graph trace from the Electrophoresis was indicative of Myeloma. However, he wants to absolutely disregard the possibility, so he is running a few more tests – one specifically for the Myeloma, and some more to check kidney function, as he also mentioned that these things can be a sign of kidneys playing up.
Again, hopefully that isn’t the case. She is passing urine with no problems like normal, and the urine itself appears to be normal in its appearance, so fingers crossed this all becomes a precautionary exercise. Necessary of course, but ultimately not telling us anything new.
He was very vocal in saying that my mother in law must be feeling like hell, given what he has seen on the bloodwork relating to her anaemia. The lab technician made a recommendation of Immunoglobulin Therapy, but this other Dr feels that he will be able to get her feeling as good as new again, once he has these final results back and knows exactly whats going on.
For reference, he has ordered the following tests:
Ferritin
Erythropoietin
PCR
C3, C4
Free Light Chains
Creatine ClearanceI believe the Free Light Chains is the final test for the Myeloma, and the rest are related to anaemia/kidney function. We are trying to get the labs ordered today, hopefully a home blood draw tomorrow, for results sometime next week. I will be sure to post back the findings, and also what the Dr is recommending for the anaemia, as and when he decides. For reference, I will post the general Bloodwork below here, which presumably denotes the state of her anaemia:
Hematocrit: 28% (ref: 38-47%)
Hemoglobin: 8g/dL (ref: 12.5-16g/dL)
Red Blood Cells: 3.31 10^6/uL (ref: 4.2-5.4 10^6/uL)
RBC distribution width: 19.1% (ref: less than 15%)
MCH: 24.2pg (ref: 27-32pg)
MCHC: 28.1pg (ref: 32-36pg)
Platelets: 551 10^3/uL (ref: 140-45010^3/uL)Thanks again guys
---
Here for my Mother In Law.
Scleroderma 30+ years, Lyme/Bartonella (perhaps 30+ years too, diagnosed in October 2019), Hypothyroid, Anemia (of chronic diseases we think?), Neuropathy, Mini-stroke/brain lesions Oct 2019, Candida.
Current Meds:
**Minocin 100mg x2 day, every day. **Rifampin 300mg 1x day MWF. **75mcg Levothyroxine. **5mg Prednisone. **Clopidogrel 75mg. **300mg Fluconazole every Sunday. **300mg Gabapentin. **LDN 4.5mg.Current Supps:
Vitamin B-complex, C, D, E. Potassium GluconaJune 4, 2020 at 10:01 pm #465802ParticipantHi Steve,
TO add to my previous post, the term free light chains was something I remember reading in my test results. The test was an Immunofixation Random Urine Test which I’m now understanding is used in patients suspected of multiple myeloma. My results read no free light chains. There doesn’t seem to be much information on a connection between Scleroderma and multiple mylemoma that I can find but it is interesting that we have similar experiences.
4/19 symptoms onset
UCTD , 1:40 ANA Speckled, Now negative
Mycoplasma P IGG IGM, EBV, HSV1, Igenix Bartonella IGG
Doxycycline 100mg b.i.d. , Bactrim ds 960 mg b.i.d. , Biodisrupt, fluconazole 100mg q.d , Monolauren, Visbiome probiotic 112.5b b.i.d ,B-complex, Vitamin D , Quercetin, saccharomyces boulardii, raw garlic , paleo, WHMJune 5, 2020 at 12:49 am #465803ParticipantSteve, forget multiple myeloma nad stop panicking. I don’t see the level of iron on your mother’s tests. It is a very important test if someone is anemic. Can you go back and see her monocytes’ levels before? How much LDN does she take?
I have read everything what you have written again and here are my conclusions. Globulin is high from blood diseases but also from the authoimmune disease and also when someone’s liver is overloaded with toxins.
I have been anemic all my life and my iron has been very low. Two years ago it was 2 and 3 /norm 7-27 uMol/L/ The body requires iron to make Hemoglobin for blood and myoglobin for muscles. Iron supplies oxygen /breathing!/and energy. Iron in excess of daily needs is stored in ferritin. I would suspect that your mother in law’s iron would be low and ferritin high. When my Hemoglobin was 8.6 doctors did an iron infusion. It was wrong and dangerous and didn’t help. Her SED is 33. Mine is now 35, what is a big improvement/it was 117 four years ago/My HCT was always low too. My platelets were 655 four years ago, now 380.
So she can have the breathing problems due to low iron. I don’t know her RDW red cell distribution width. Maybe it is increased. It should be checked. A low haematocrit HCT with a low MCV mean corpuscular volume and a high RDW would suggest a chronic iron deficient anemia. It is important to check which anemia she has
Sorry I am comparing my results to hers but I don’t want you to think the worst too early. I have learnt, like many of us here, not to trust the doctors. Too many of them want us to be sick. I witnessed a case of an elderly lady a year ago, when her doctors made three times tests /three biopsies/towards cancer and they were negative. After that she was forced to undergo the radiation.
I think also that she is overloaded with the toxins from many medications and supplements and she cannot cope with that.
I took my last Prednisone four years ago. I was taking it long time together with Methotraxate. I started a struck diet. No gluten and no dairy. I started a LDN two years ago and I take it until now. I take Mobil every third day and NDT for thyroid. My last results six months ago – Hemoglobin 11.9 and iron 7, platelets 380, SED 35. It doesn’t mean that I don’t suffer with arthritis, I do, but my nervous system, brain, confidence, energy are much better now.RA tried everything: Methotraxate, Arava, Humira. Pneumonia three times. Anemia. Very low iron. Hypothyroidism
AP from April 2014 till August 2015. No luck.
Current medications: Natural thyroid, Mobic, supplements,
vitamins and minerals.
MTHFR heterozygousJune 5, 2020 at 1:31 am #465804ParticipantI have noticed some mistakes in my previous message. Strict diet of course. I take Mobic. Mobil would be too oily.
It’s not me. If I don’t check, my computer changes the letters…RA tried everything: Methotraxate, Arava, Humira. Pneumonia three times. Anemia. Very low iron. Hypothyroidism
AP from April 2014 till August 2015. No luck.
Current medications: Natural thyroid, Mobic, supplements,
vitamins and minerals.
MTHFR heterozygousJune 5, 2020 at 8:34 am #465805ParticipantThanks both of you for your further replies!
Vincent, yes it is interesting. I suppose along the way labs between patients may resemble one another, but as we all know things can be equally so varied from patient to patient, and furthermore anomalies can crop up that, in the end, are all part of the same process/condition. Thanks for sharing your experiences, we at least feel a little more calm that she shares this process with other people like yourself!
Linda, its so great to read of such a huge improvement you’ve had in your bloodwork. More importantly, though, that you actually feel better. As my wife and I always say, my MIL has what she has, results or no results. It’s a part of life nobody can really control. But what all these test results do mean is that we can make the correct decisions together to help her feel better.
It’s funny, for the past year we have really helped her improve her diet. No more sugar, artificial flavours/sweetners (only Stevia), cut out the Gluten, etc, and there has been a marked improvement. However this week, we went a bit further to cut out all meats (including chicken). We knew before that red meats can be inflammatory, but we saw an interesting video the other day suggesting that chicken could be too. This week, it has been salads, loads of vegetables, and fish (no shellfish). Remarkably (or perhaps not quite so remarkably), she has been visibly better. More energy, happier, a little less pain due to her neuropathy. Still tired and dizzy, but other aspects are definitely improving. We’re going to see how far the diet can take her (it helps that her daughter/my wife is an amazing pair of hands in the kitchen of course!!)
She is getting the blood drawn on Monday, so will be sure to report back.Ferritin levels are being checked, I’ll make sure that Iron is also on the list.
Linda I see you say you stopped Prednisone 4 years ago. Thats really amazing, we’ve read countless times the damage that prednisone can do to you, and how it can really screw with the balance of things in your system. We have been saying for a long time how great it would be to help her wean off it… Just over a year ago, she was taking 10mg Pred and 75mg Diclofenac every day, and still in a lot of body-wide inflammation pain etc. Today, she takes 5mg Prednisone and 1/4 of the 75mg Diclofenac tab (roughly 18mg I guess). And her pain is so much better. No more trips to the hospital for inflammation-related pain, or trips to the slightly dodgy chemist for Diclofenac injections! Neuropathy pain persists, but that is a bit of a separate issue…
How did you go about stopping Pred? We’ve read it can be dangerous to stop cold turkey, and we remember that dropping from 10mg-5mg was pretty tough on her, although she has now adjusted. Perhaps she isn’t quite ready to do that yet, but it would be great to know how you went about it, so that when she perhaps feels she is ready, we can try ourselves.. Again, the trouble here is that her Rheumy here in Ec will only ever prescribe Prednisone and Diclofenac (thats all she has ever done for the past 10 years or so…) so the idea of coming off it would just not sit with her Dr here AT ALL.
Just finally on the trust of Drs – we completely agree with this notion. I always fear of coming across as someone who thinks they ‘know it all’, which couldn’t be further from the case. We try and learn everything we can, so we can also form rational decisions as human beings, to know whats best for my Mother In Law. As I’ve expressed before, it was my wife and I that sent MIL’s blood from Ecuador to US to get checked for Lyme, the Drs here would never dream of doing it (nor had it ever really occurred to them). Upon receiving the positive results, the Rheumy’s comments were this to my wife (along these lines):
‘Well, I think that I’m the Dr here so I should make the decisions on how to approach your mom’s condition. I’m going to treat what it’s clear she has, and it’s obvious that she has Scleroderma, dont you think? So that’s what I’ll treat…’
Also, whilst suffering from her mini-lesions on her brain, the A&E doctors turned her away. Unconvinced, we went to get her scanned privately, and returned the next day with the scan results. The A&E guys STILL wanted to turn her away. Thankfully, a neurologist was working that night, and he took a look at the scans, and then insisted she come in to the hospital…
Two separate circumstances, but highlights the negligence/borderline incompetence/ignorance/arrogance that can be faced with Drs (not that uncommon over here unfortunately). Hence our general lack of belief in the Drs here. Thankfully we have a great one now in the US, but I always feel that real patient testimonies like everyone on this forum lead the way to really getting to the bottom of what is going on!
---
Here for my Mother In Law.
Scleroderma 30+ years, Lyme/Bartonella (perhaps 30+ years too, diagnosed in October 2019), Hypothyroid, Anemia (of chronic diseases we think?), Neuropathy, Mini-stroke/brain lesions Oct 2019, Candida.
Current Meds:
**Minocin 100mg x2 day, every day. **Rifampin 300mg 1x day MWF. **75mcg Levothyroxine. **5mg Prednisone. **Clopidogrel 75mg. **300mg Fluconazole every Sunday. **300mg Gabapentin. **LDN 4.5mg.Current Supps:
Vitamin B-complex, C, D, E. Potassium GluconaJune 5, 2020 at 9:38 am #465806Lynne G.SD
ParticipantHi Steve;
Are you aware that the Lyme can cause those brain lesions?June 5, 2020 at 9:46 am #465807ParticipantDang,this did not attach.
https://globallymealliance.org/living-lyme-brain/June 5, 2020 at 7:23 pm #465808ParticipantDoes she take LDN? How much and since when?
RA tried everything: Methotraxate, Arava, Humira. Pneumonia three times. Anemia. Very low iron. Hypothyroidism
AP from April 2014 till August 2015. No luck.
Current medications: Natural thyroid, Mobic, supplements,
vitamins and minerals.
MTHFR heterozygousJune 6, 2020 at 8:55 pm #465809ParticipantI was taking 5 mg Prednisone. I started to take 5-5-4, so every third day I was taking less for two weeks, then for two weeks 5-4-5-4, then 5-4-4, then 4, then 4-4-3 and so on.
RA tried everything: Methotraxate, Arava, Humira. Pneumonia three times. Anemia. Very low iron. Hypothyroidism
AP from April 2014 till August 2015. No luck.
Current medications: Natural thyroid, Mobic, supplements,
vitamins and minerals.
MTHFR heterozygousJune 6, 2020 at 11:48 pm #465810ParticipantThanks guys for your continued support.
Lynne – yes we are aware of this. It was quite a set of events, she was in hospital due to these 4 small lesions on her brain (still undiagnosed for Lyme). We were reading late one night trying to see why this happened, and we came across an article referencing brain lesions and Lyme! That coupled with the neuropathy, led us to get her tested (positive!) The drs here did every test possible, and couldn’t determine why the lesions happened. Therefore standard procedure meant they prescribed her blood thinners and that was that! We believe the neuropathy and lesions are both due to the Lyme.
Linda – she first started LDN last March (ie 14 months ago). We were experimenting with dosage, trying to determine the best. However the stroke/lesions then hit, so she stopped taking it.
She restarted again a few months ago, but just last week ran out… we can’t get it here in Ecuador, so we got an order coming from the U.K. later this month.
On this most recent run, she was taking 3mg at night. I’m aware everyone has a different optimal dose, but a lot tend towards the 4.5mg end. We shall see when we get the new batch…
As for prednisone, that’s so great you got off it, and makes sense how you went about it. Our problem (yet again) is that the smallest dosage they stock is 5mg, and it’s a tiny pill. Cutting it would be a waste of time, and so inaccurate that it would not be safe at all. Is there a way of dissolving it in a set amount of liquid to split up the dose that way perhaps?
---
Here for my Mother In Law.
Scleroderma 30+ years, Lyme/Bartonella (perhaps 30+ years too, diagnosed in October 2019), Hypothyroid, Anemia (of chronic diseases we think?), Neuropathy, Mini-stroke/brain lesions Oct 2019, Candida.
Current Meds:
**Minocin 100mg x2 day, every day. **Rifampin 300mg 1x day MWF. **75mcg Levothyroxine. **5mg Prednisone. **Clopidogrel 75mg. **300mg Fluconazole every Sunday. **300mg Gabapentin. **LDN 4.5mg.Current Supps:
Vitamin B-complex, C, D, E. Potassium GluconaJune 7, 2020 at 12:41 am #465811ParticipantHi Steve,
we have 1 mg pills here but when it came to the final crunch I just used a nail file to shave a bit off until managing to get off of it.June 7, 2020 at 1:23 am #465812ParticipantTry to speak to your pharmacist about Prednisone.
RA tried everything: Methotraxate, Arava, Humira. Pneumonia three times. Anemia. Very low iron. Hypothyroidism
AP from April 2014 till August 2015. No luck.
Current medications: Natural thyroid, Mobic, supplements,
vitamins and minerals.
MTHFR heterozygous -
AuthorPosts
{kind=link}
{kind=link}
{kind=link}
You must be logged in to reply to this topic.